We Forced Our Teen Daughter to Give Up a Kidney. She Grew Up to Be a Surgeon—and Now She Won’t Save Us.
There are moments in life that split time into before and after—moments so profound that they mark the boundaries of who we once were and who we become. For our family, that moment came not in the operating room, nor in the tense silence of a hospital waiting area, but in a hallway, years later, as Dr. Emily Lang strode past the chaos of her father’s heart attack and did nothing.
To the nurses, she was a rising star—a trauma surgeon whose skill and composure saved countless lives. To us, she was the daughter we had once forced to save her sister, the child whose body we had claimed for the sake of another’s survival. As I watched her walk away, the shame that knotted in my stomach was more painful than any grief I had ever known. In that instant, I understood: some wounds do not heal, and some choices, made in the name of love, exact a price that cannot be repaid.
This is the story of our family—a story of sacrifice, coercion, and the irrevocable consequences of believing that love justifies any act. It is a story about what happens when the boundaries between care and control blur, when desperation overrides ethics, and when the act of saving one child costs you another. Through the lens of Emily’s journey—from forced donor to accomplished surgeon, from daughter to stranger—this essay seeks to unravel the complex tapestry of trauma, guilt, and loss that defines our family, and to ask what it truly means to save someone.
II. The Decision: Sacrifice and Coercion
When Lily fell ill, the world narrowed to the sterile confines of hospital rooms and the relentless tick of monitors. She was young, vibrant, the kind of child whose laughter filled every corner of our home. Her diagnosis—chronic kidney disease, rapidly progressing—was a blow that left us gasping, scrambling for solutions. The doctors spoke in probabilities and percentages, but the message was clear: without a transplant, Lily’s future was measured in months, not years.
We were desperate. In that desperation, we turned to Emily.
At seventeen, Emily was quiet, thoughtful, a girl who kept her emotions folded away like secrets. She was healthy. She matched. The doctors explained the risks, the recovery, the possibility of complications. They spoke of consent, of the importance of understanding. But in the haze of fear and hope, those words became background noise. We saw only Lily’s fading color, her weakening voice, and the chance—however slim—to save her.
The conversation that followed remains etched in my memory, a tableau of pleading and resistance. Emily sat on the edge of her hospital bed, hands clenched in her lap, eyes wide with something I later recognized as terror. We told her it was the right thing to do, that Lily needed her, that families made sacrifices for one another.
She asked if she had a choice.
We told her she did—but our voices betrayed us. The truth was, we could not imagine another way. In our minds, Emily’s kidney was not hers alone; it was the lifeline that would keep Lily alive. The doctors required her assent, but we required her compliance. The line between consent and coercion blurred, then vanished.
Emily agreed. Or rather, she surrendered.
The surgery was successful. Lily’s body accepted the graft, and for a time, hope bloomed in our hearts. But beneath that hope lay the seeds of something darker—a resentment that would grow, quietly, relentlessly, until it eclipsed every other feeling.
III. The Aftermath: Family Dynamics and Emotional Fallout
Recovery was a process measured not just in days and weeks, but in fractured relationships and unspoken words. Emily healed physically, but emotionally, she withdrew. The girl who had once been so open became guarded, distant. She stopped coming to family dinners, spent hours alone in her room, and when she spoke, her words were clipped, careful.
Lily, meanwhile, thrived. Her color returned, her energy rebounded, and she resumed the rhythms of adolescence. But the shadow of the transplant hung over her, an unspoken debt she could never repay. She sensed Emily’s withdrawal, felt the distance growing between them, and responded with guilt—a guilt that would shape her for years to come.
As parents, we rationalized. We told ourselves that time would heal, that Emily would come to understand, that Lily’s gratitude would bridge the gap. But beneath our optimism lurked a gnawing fear: that we had asked too much, that our love had become a kind of violence, that we had broken something that could not be mended.
The silence in our home became a presence, heavy and suffocating. Emily graduated high school, left for college, and rarely called. Lily grew older, her health stable but always precarious. We learned to live with the absence, to fill the void with routine and denial.
But the rupture was permanent. The family we had once been—a unit bound by love and laughter—had become a collection of individuals, each nursing their own wounds.

IV. Emily’s Transformation: From Victim to Surgeon
Despite—or perhaps because of—her experiences, Emily chose to study medicine. It was a decision that surprised us, one we interpreted as a sign of healing. We imagined her driven by compassion, by a desire to save others as she had saved her sister. But as the years passed, it became clear that Emily’s motivation was not empathy, but control.
She excelled, rising quickly through the ranks of her residency, earning praise for her skill and composure. But she remained emotionally distant, her bedside manner professional but impersonal. She treated patients with efficiency, never lingering, never allowing herself to be drawn into their stories.
The moment that crystallized the extent of her detachment came during her father’s heart attack. Rushed to the hospital, we found ourselves in the chaos of the ER, surrounded by doctors and nurses. Emily appeared, her presence commanding, her reputation preceding her. But when she saw us, she turned away, refusing to assist, refusing even to acknowledge our pleas.
The nurses were confused. We were devastated.
My husband survived, but the damage was done. For days, he said nothing, until finally, he whispered, “She really hates us, doesn’t she?” I could not bring myself to answer. The truth was too painful to admit.
V. The Family’s Response: Shame, Guilt, and Grief
In the aftermath, we tried to reach out. Letters, emails, messages through friends—all met with silence. Emily had severed ties, and no amount of apology or explanation could bridge the gap.
When Lily’s condition worsened, we hoped—desperately—that Emily might reconsider. We called, pleaded, begged. Emily’s response was cold, final: “I gave up a part of my body for her. That’s more than enough.”
The line went dead.
Lily cried, wracked with guilt and grief. She understood, finally, the true cost of her survival. “She hates me,” she sobbed. I tried to comfort her, but my words rang hollow. Emily’s anger was more than hatred—it was a refusal to be defined by the family that had betrayed her.
We sent a certified letter. It came back unopened.
Lily spent weeks in intensive care, her future uncertain. One night, she asked the question I had feared: “Did she ever want to save me?” I could not answer. The truth was too heavy, too complex for words.
VI. Ethical Analysis: Medical Consent and Familial Responsibility
The ethics of organ donation are clear: consent must be informed, voluntary, free from coercion. But in the crucible of family crisis, those principles are often tested, bent, broken. We believed that love justified our actions, that the bond between siblings made Emily’s sacrifice noble, even necessary.
But love cannot erase the violation of autonomy. The psychological consequences of forced donation are profound—resentment, guilt, trauma that lingers for years. For Lily, survival came at the cost of her relationship with her sister. For Emily, the loss was deeper: a sense of agency, trust, and belonging.
As parents, we failed to protect both our daughters. We allowed desperation to override ethics, and in doing so, we inflicted wounds that medicine could not heal.
VII. Healing and Acceptance: Lessons Learned
In time, we learned to accept the permanence of the damage. Lily stabilized, growing older and wiser, carrying the guilt of survival. My husband rarely spoke of Emily, his silence a tacit admission of our failure.
We heard, through friends, that Emily had taken a teaching position at a university hospital. She had built a life apart from us, a life defined by her own rules, her own boundaries.
We did not try to contact her again.
The family we had once been was gone, replaced by a fragile peace. We learned to live with the absence, to find meaning in the fragments that remained.

VIII. Conclusion
The story of Emily and Lily is a cautionary tale—a reminder that love, when twisted by desperation, can become a kind of violence. The cost of coerced sacrifice is measured not just in bodies, but in souls, in relationships irreparably damaged. As parents, we must reckon with the boundaries of our authority, the limits of our love.
Emily survived her surgery, became a surgeon, and built a life apart from the family that broke her. Lily survived, but carries the weight of her sister’s resentment. And we, their parents, live with the knowledge that some choices cannot be undone.
In the end, a daughter can survive a surgery—and still never come home again.
News
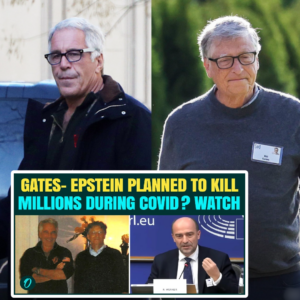
‘Gates, Epstein Had a Plan?’ Economist’s Explosive Claims About ‘Ending Poverty by 2020’ Spark Shock
Explosive Allegations: Economist Links Gates and Epstein to Ambitious Poverty Plan — Sparks Outrage The Epstein-Gates Connection: Economist Exposes 2017 “Great Pandemic” Plot and the Global Push for Total Digital Control In a revelation that has sent shockwaves through the…

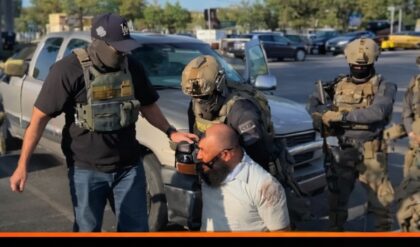
Breaking: Missing Crew Member From Crashed U.S. Fighter Jet Recovered
After Tense Search, Missing Crew Member From Downed Fighter Jet Reportedly Rescued Rescue Under Fire: US Special Forces Extract Downed Airman as Trump Issues 48-Hour “All Hell” Ultimatum to Iran The geopolitical landscape of the Middle East has shifted into…

BREAKING: Downed F-15 Crew Member Rescued in Iran as War Intensifies
Daring Rescue Behind Enemy Lines: F-15 Crew Member Saved Amid Escalating War Miraculous Rescue in the Midst of Chaos: US Special Forces Extract Downed F-15E Colonel After Brutal Firefight in Iranian Mountains In what is being described by military analysts…

DOJ Unleashes Major Crackdown on California’s ‘Fraud Kingdom’ in $60M Hospice Bust
Massive Takedown: DOJ Moves Against California’s Alleged ‘Fraud Kingdom’ in $60M Case Operation “Never Say Die”: DOJ Crushes $60M “Kingdom of Fraud” in California as Federal Task Force Targets Corrupt Hospice Networks In a dramatic show of force that marks…
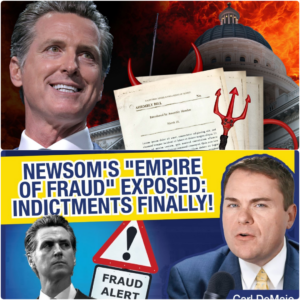
Breaking: Indictments Emerge Amid Explosive ‘Empire of Fraud’ Claims Against Newsom
‘Empire of Fraud’ Allegations Rock Gavin Newsom — Indictments Finally Surface California’s “Empire of Fraud” Unmasked: Federal Indictments Begin as Billions in Taxpayer Funds Vanish Under Newsom’s Watch For years, a “ragged, ratchety sweater” of corruption has been quietly unraveling…

REPLAY: General Ousted After Challenging Hegseth on Black Promotions
Tensions Explode as Hegseth Fires General Who Questioned Promotion Decisions The Pentagon Purge: Hegseth Accused of Blocking Black and Female Promotions to Cement a “White Men Only” Military Leadership The United States military has long prided itself on being one…
End of content
No more pages to load