“I Can’t Breathe” – A 18-Year-Old German POW Boy Arrived With Punctured Lung – Doctors SHOCKED D
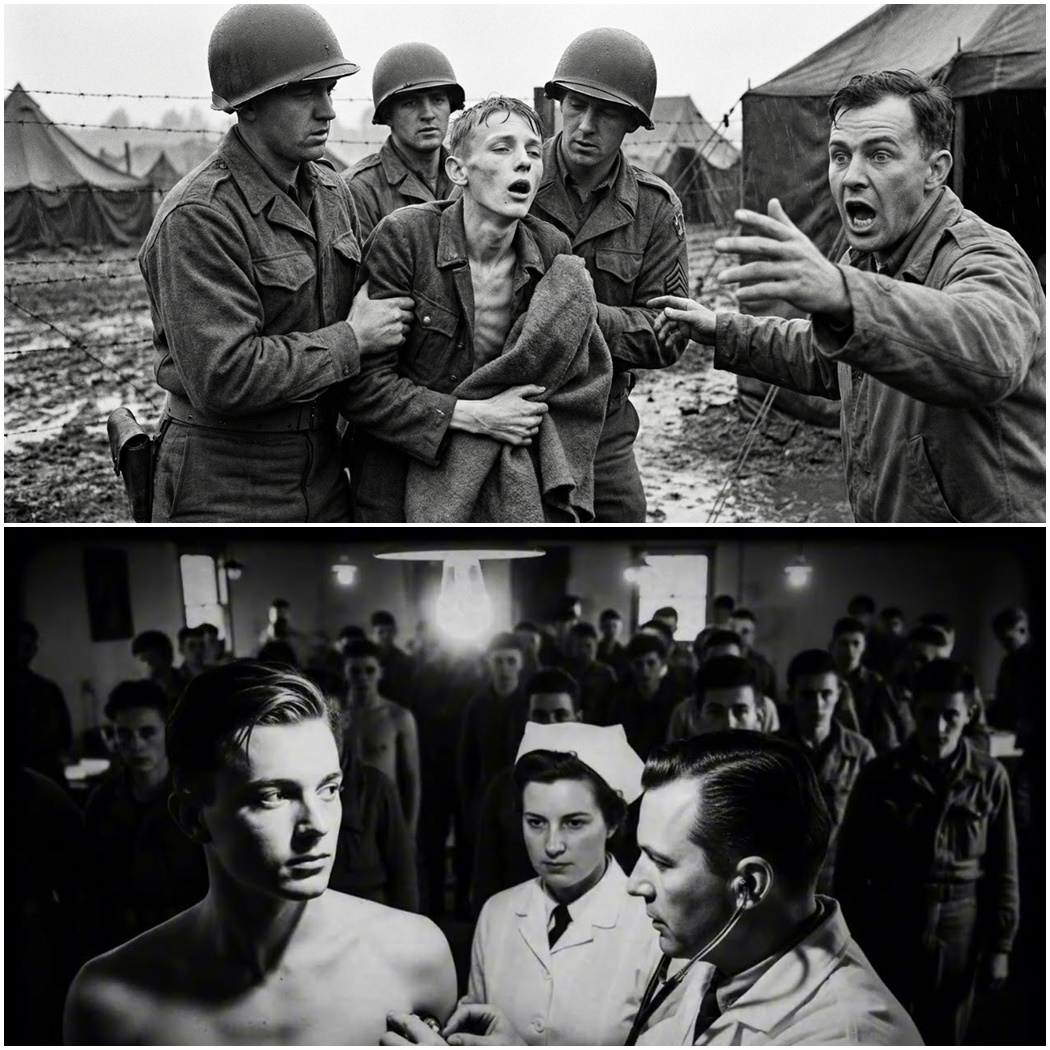
The boy is 18 years old. He is standing in front of an American military doctor in a prisoner of war processing station somewhere in France in late 1944. He is not screaming. He is not crying. But every breath he takes sounds like wet paper tearing inside his chest. The doctor leans closer and listens again.
That sound should not be coming from a living person. The doctor looks at the nurse and says three words that will change everything for this boy. Get him inside now. We are in a field hospital near the FrancoGerman border in November 1944. The war is closing in on Germany from both sides.
Allied forces are pushing east. Soviet forces are pushing west. German units are collapsing, surrendering, or retreating in chaos. In the middle of this, prisoners of war are flooding into Allied processing stations by the thousands every single day. Most of these prisoners arrive in predictable conditions, exhausted, malnourished, lice ridden, dehydrated.
The medical staff have seen it all before. They process them quickly. Check for typhus, scabes, tuberculosis, delousing station, food, interrogation, transport to a permanent camp. It is a factory line designed for volume, not individual cases. But this boy breaks the pattern. He arrives on foot with a column of about 200 German prisoners captured near the Huichin forest.
The guards march them into the camp perimeter. Roll call, document check, basic medical screening. The boy stands in line like everyone else. But when the nurse tells him to step forward and breathe deeply, she hears it. a sound like air escaping through water. She freezes. She calls the doctor over. He listens. He hears it, too.
That sound means the boy should be dead or unconscious or at least on the ground, but he is standing. The doctor asks him a question in broken German. How long has this been happening? The boy does not answer right away. He looks at the ground. He looks at the nurse. Then he says in quiet German that the translator repeats in English.
Since the transport, the doctor asks another question. What transport? The boy says the cattle cars three days ago. The doctor writes something on a clipboard and signals two medics. They take the boy by the arms and walk him toward the medical tent. The other prisoners watch in silence. Some of them know what happened to him.
None of them thought he would make it this far. We are inside the medical tent now. The boy is sitting on a cot. The doctor is standing in front of him with a stethoscope. The nurse is preparing bandages and instruments on a metal tray. The boy is still breathing that wet tearing sound. Let us pause here and explain what is actually happening inside his body.
Because this is not a simple injury. This is a trauma that most soldiers do not survive in the field. A punctured lung means that the plural cavity, the sealed space around the lung has been breached. Air is leaking into that space with every breath. The lung is collapsing partially or fully. The pressure inside the chest is building.
This condition is called pneumothorax. In severe cases, it becomes tension pumothorax where the pressure builds so much that it compresses the heart and the other lung. Death follows in minutes. The boy is not at that stage yet, but he is close. The symptoms are unmistakable. Rapid shallow breathing. Sharp chest pain on one side. A sucking sound when air moves through the wound.
Bluish skin tone from lack of oxygen. Confusion or dizziness. Rapid heart rate. The boy has most of these. His lips are pale. His fingernails are slightly blue. His heart is racing at over 120 beats per minute. But he is conscious. He is answering questions. He is still standing when most people with this injury would be flat on their back gasping for air and begging for help.
The doctor removes the boy’s shirt. There it is, a wound on the left side of his rib cage just below the armpit. The skin around it is bruised, dark purple, and yellow. The wound itself is about 3 cm long. It is not bleeding heavily anymore, but every time the boy inhales, the doctor can see the tissue move.
Air is going in and out through the hole. The doctor presses gently around the wound. The boy flinches but does not cry out. The doctor looks at the nurse and says one word, “Shrapnel.” The nurse nods, but the doctor is not satisfied with that answer yet because shrapnel wounds usually happen in combat and this boy was captured days ago.
So, what actually happened? The doctor sits down on a stool next to the cot and asks the boy to explain. The translator is standing nearby. The boy starts talking. His voice is low and he pauses every few sentences to catch his breath. This is what he says. He was part of a vermached infantry unit assigned to defend a supply route east of Aken.
The unit was overrun by American forces on November 7th, 1944. He and about 40 other soldiers were captured and held in a temporary enclosure for two days. No shelter, no food except one meal of bread and soup. Then they were loaded onto cattle cars for transport to a larger prisoner of war processing camp in France.
The cattle cars were the same ones used for livestock and freight. Wooden floors, metal walls, no windows except small barred openings near the roof. Each car was packed with 60 to 80 men. The boy was in the middle of the car with no space to sit down. Everyone was standing or crouching. The train started moving. It stopped and started over and over again.
Air raids, track damage, refugee traffic. The journey that should have taken one day stretched into three days. No food, no water, one bucket in the corner for waste. The smell was unbearable. Men were fainting. Some were crying, others were silent. On the second night, the train stopped suddenly. Then they heard it.
Aircraft engines. The men in the car started shouting. Some pounded on the walls. The guards outside ran for cover. Then the explosion started. Allied planes were strafing the train. Rockets, machine gun fire. The cars were not marked as prisoner transport. From the air, it looked like a military supply train. The boy says he does not remember the exact moment he was hit.
He remembers a loud crack, a flash of light through the gap near the roof, then pressure in his chest, then wetness. He looked down and saw blood spreading across his shirt. He put his hand on the wound and felt air bubbling out. The men around him tried to help. One of them tore a piece of cloth from his own shirt and pressed it against the wound, but there was no medic, no bandages, no morphine.
The train started moving again after the planes left. The boy stayed on his feet because there was no room to lie down. He pressed the cloth against his ribs and focused on breathing. Slow and shallow. Do not panic. Do not scream. Screaming uses air. Air was the one thing he could not afford to waste. He stayed like that for another full day and night until the train reached the processing station.
When the doors finally opened and the guards ordered everyone out, the boy climbed down and walked into the camp with the others. Nobody noticed. He was injured until the medical screening. The doctor finishes listening to the boy’s story. He looks at the nurse. He looks at the translator. Then he looks back at the boy and says something in English that the translator does not repeat.
This should not be possible. But let us step back and ask the question that the doctor is asking. Why is this boy still alive? Because by every medical standard, he should not be. Let us go through the factors one by one. First, the wound was small. The piece of shrapnel that punctured his lung was not a large fragment.
It entered at an angle, penetrated the plural cavity, nicked the lung tissue, and exited or stayed shallow. A larger wound would have caused massive air leakage and immediate collapse. A smaller wound would have sealed itself. This wound was in the narrow zone where the body could partially compensate. Second, he stayed upright.
If he had laying down in the cattle car, the pressure distribution in his chest would have worsened. Staying vertical helped keep the uninjured lung functional. Third, he controlled his breathing. Panic breathing would have accelerated the collapse. He breath slowly and shallowly, which limited the air pressure differential.
Fourth, he pressed cloth against the wound. This created a partial seal, not perfect, but enough to reduce the air flow in and out. Fifth, he was 18 years old. His body was young and resilient. His cardiovascular system compensated for the reduced oxygen by increasing his heart rate. Older prisoners of war would not have survived the same injury under the same conditions.
But there is one more factor. Luck. The shrapnel missed his heart by centimeters. It missed the major blood vessels in his chest. It did not fragment further inside his body. If any of those variables had been different, he would have bled out in the cattle car and been unloaded as a corpse. The doctor knows this.
The nurse knows this. And now the boy is sitting in front of them, still breathing that terrible wet sound, waiting to find out if anyone can actually fix him. Let us know in the comments where you are watching this from. Are you in the United States, Germany, the United Kingdom, or somewhere else. We would love to know who is keeping these stories alive.
Now, back to the tent because the doctor is about to make a decision that will determine whether this boy lives or dies. We are still in the medical tent in November 1944. The boy is on the cot. The doctor has made his assessment. The lung is partially collapsed. Air is leaking into the plural space. The wound needs to be sealed.
The pressure needs to be released. If they do nothing, the boy will die within 24 to 48 hours. If they try to treat him here with limited supplies and no surgical team, he might die anyway, but doing nothing is not an option. The doctor explains the plan to the nurse. They are going to perform a needle decompression first to release the builtup air pressure.
Then they will clean and seal the wound. Then they will insert a chest tube to allow ongoing drainage and prevent ray collapse. This is field medicine. It is not a hospital. There is no operating room. No anesthesia except local morphine. No blood transfusions. No x-ray to confirm placement. The doctor has done this procedure twice before.
Both times on American soldiers injured in combat. One survived, one did not. The boy will be the first prisoner of war he has attempted this on. The nurse prepares the supplies. A large bore needle, a scalpel, sterile gauze, a rubber chest tube, a glass bottle with a water seal valve, morphine. The doctor injects morphine into the tissue around the wound. The boy closes his eyes.
The doctor waits 2 minutes. Then he takes the needle and inserts it into the second intercostal space on the left side of the boy’s chest just below the collar bone. There is a hiss of air escaping. The boy gasps. His breathing immediately becomes less strained. The pressure has been released. The doctor removes the needle and moves to the wound itself.
He cleans the wound with antiseptic. The boy flinches but stays still. The doctor examines the entry point. The shrapnel is not inside the wound anymore. It either fell out or passed through. That is good. No foreign object to remove. The doctor packs the wound with gauze soaked in antiseptic and covers it with a pressure bandage. Then he makes a small incision between the ribs lower down on the boy’s chest.
He inserts the chest tube carefully, advancing it into the plural space. The boy groans. The nurse holds his shoulder. The doctor connects the tube to the glass bottle. Immediately, air and a small amount of blood start bubbling through the water seal. The lung is draining. The doctor tapes the tube in place and wraps the boy’s chest with bandages to hold everything secure.
The procedure is finished. The boy is still conscious. His breathing is quieter now. The wet tearing sound is gone. His heart rate is starting to drop. His skin color is improving. The doctor tells the nurse to monitor him every 2 hours. No food yet. Water only in small sips. If the boy develops fever, confusion, or worsening breath sounds, they will reassess.
The boy lies back on the cot. He closes his eyes. For the first time in three days, he is not fighting for every breath. The doctor walks out of the tent and lights a cigarette. He does not know yet if the boy will survive, but he has bought him time. If you are enjoying this story and want more untold accounts from World War II prisoners of war, make sure to subscribe to the channel.
We are bringing you stories that most history books never covered. Now let us move forward because the boy’s survival depends on what happens in the next 72 hours. We are now tracking the boy’s condition over the next 3 days. Time is critical. Pumothorax survivors face multiple complications. Infection is the biggest risk.
The wound was contaminated in the cattle car. The chest tube is an entry point for bacteria. The boy’s immune system is already weakened by malnutrition. dehydration and stress. If infection sets in, it will spread to the plural cavity and become empa, a collection of pus around the lung. Empa is almost always fatal in field conditions. The doctor knows this.
So does the nurse. They are watching for fever, foul smelling drainage, and increased pain. Hour 12. The boy is awake. His breathing is steady. The chest tube is draining small amounts of clear fluid mixed with blood. That is normal. The nurse gives him water. He drinks slowly. No vomiting, no choking. His lung is expanding.
The doctor listens with the stethoscope. Breath sounds are present on both sides now, but the left side is still diminished. The lung has not fully ray inflated yet. The doctor makes a note on the chart. Continue monitoring. No signs of infection yet. Hour 24. The boy is sitting up. His color is better. His heart rate is down to 90 beats per minute. Still elevated but improving.
The nurse changes the bandages. The wound looks clean. No pus. No red streaks. The boy asks for food. The doctor says, “No, not yet. Not until we are sure your body can handle it.” The boy does not argue. He lies back down. He sleeps for 4 hours straight. That is the first real sleep he has had since the cattle car. Sleep is healing.
The body repairs itself during rest. The doctor allows it. Hour 48. The boy is standing. He takes a few steps around the tent. The chest tube is still in place connected to the drainage bottle. He moves carefully holding the bottle with one hand. The nurse watches him. He does not fall. He does not gasp for air.
His lung is working. The doctor examines him again. Breath sounds are nearly equal now. The drainage has slowed to a trickle. The wound is dry. No fever. The boy is past the immediate crisis, but he is not out of danger yet. The doctor decides to keep the chest tube in for another 24 hours.
If the lung stays inflated and no infection develops, they will remove the tube and transfer the boy to a regular prisoner of war camp with a medical barracks. Hour 72. The doctor removes the chest tube. The boy lies on his side. The nurse holds his hand. The doctor pulls the tube out in one smooth motion. The boy grunts.
The doctor stitches the incision closed and applies a fresh bandage. It is done. The boy’s lung is ray inflated. The wound is sealed. He has survived. The doctor writes a note in the boy’s medical file. Pumothorax secondary to shrapnel injury. Treated with needle decompression and chest tube insertion. No complications.
Stable for transfer. The boy will be moved to a camp in eastern France within 2 days. From there he will eventually be transferred to a larger permanent camp possibly in the United States or the United Kingdom but that is a different story. Let us pause here and talk about the scale of medical treatment for prisoners of war during World War II because the boy’s case was not unique in terms of injury.
It was unique in terms of survival. Thousands of prisoners of war arrived at Allied processing stations with untreated wounds from combat, transport or camp conditions. Most of them did not receive the level of care that this boy received. Let us look at the numbers. By the end of 1944, the Allies were capturing German prisoners of war at a rate of over 50,000 per month on the Western Front alone.
Medical resources were stretched thin. Priority was given to Allied soldiers first, then to prisoners of war based on severity and likelihood of survival. A prisoner with a minor wound might wait days for treatment. A prisoner with a fatal wound might receive only morphine and comfort care. The boy fell into a narrow category. Severe injury but survivable with immediate intervention.
That combination saved his life. Pumothorax had a mortality rate of about 30 to 40% in field conditions during World War II, even with treatment. Without treatment, the mortality rate was over 80%. The boy survived because he received care within hours of arrival. Most prisoners of war injured during transport never made it to a medical tent.
They died in the cattle cars, in the trucks, or in the holding pens before anyone noticed. The exact number is unknown, but estimates suggest that between 5 and 10% of prisoners of war died during transport between capture and arrival at a permanent camp. That is tens of thousands of men across all theaters of the war.
Chest wounds specifically were among the deadliest injuries for prisoners of war. Shrapnel, bullet fragments, broken ribs from beatings or overcrowding. All of these could puncture a lung. Allied doctors treated hundreds of cases like the boys during the final year of the war. Survival depended on timing, skill, supplies, and luck. The boy had all four.
Most did not. By the time the war ended in May 1945, Allied forces had processed and treated over 5 million German prisoners of war in Western Europe alone. Medical records from that period show that respiratory injuries, including pneumothorax, accounted for approximately 8% of all prisoner of war medical cases.
Of those cases, fewer than half survived beyond the first week. We are now in late November 1944. The boy has been transferred from the field hospital to a prisoner of war camp in eastern France near the town of Apinnel. This camp holds about 3,000 German prisoners. Most of them are infantry soldiers captured during the autumn offensives.
The camp has a medical barracks with two doctors and six nurses. The boy is assigned to a bed in the recovery section. His chest is still bandaged. He is not allowed to do heavy labor yet. The doctors want to monitor him for another 2 weeks to make sure no complications develop. The boy’s days in the camp are simple.
Wake up at 6:00 in the morning. Roll call. Breakfast of bread, margarine, and airsoft coffee. Rest in the barracks. Lunch at noon. More rest. Dinner at 6:00. Lights out at 9:00. He is not in pain anymore. The wound is healing. He can breathe normally. He can walk without dizziness. But he is still weak. His body is recovering from the injury, the blood loss, and the weeks of malnutrition before capture.
He eats every meal slowly and carefully. He drinks water whenever it is available. He sleeps 10 hours a day. Recovery is not dramatic. It is boring. But boring means alive. The other prisoners in the barracks ask him about the wound. He tells them the story of the cattle car. Some of them were on the same train. They remember the air raid.
They remember the explosions. They did not know anyone had been hit until now. One of the older prisoners, a sergeant in his 30s, tells the boy he is lucky. The sergeant says he saw a man with a similar wound die in less than an hour during the retreat from Normandy. The boy does not feel lucky. He feels tired, but he is alive and that is enough for now.
By mid December 1944, the boy is cleared for light work duty. He is assigned to the camp kitchen, peeling potatoes, washing dishes, carrying supplies. It is not hard labor, but it keeps him occupied. The camp is relatively well-run compared to some of the stories he has heard from other prisoners. There is enough food. There is shelter.
There is no brutal punishment. The guards are mostly older American soldiers who do not care about ideology. They just want the war to end. The boy works in the kitchen through the winter. He gains weight. His strength returns. By February 1945, he looks like a normal 18-year-old again. The scar on his chest is the only reminder of what happened in the cattle car.
Let us step back and put the boy’s story into context. Because the way the Allies treated German prisoners of war in the final years of World War II was shaped by a combination of international law, logistics, and pragmatism. The Geneva Convention of 1929 set the rules. Prisoners of war must be treated humanely.
They must receive adequate food, shelter, and medical care. They must not be subjected to torture or degrading treatment. They must be allowed to send and receive mail. They must be released or repatriated after the war ends. The Allies generally followed these rules, especially on the Western Front. But there were exceptions.
The biggest challenge was scale. By 1945, the Allies were holding millions of German prisoners of war. The camps were overcrowded. Supplies were limited. Medical staff were overwhelmed. Some prisoners received excellent care, like the boy in this story. Others received minimal care or none at all. The difference often came down to timing and location.
Prisoners captured early in the war and sent to camps in the United States or Canada generally had better conditions than prisoners captured late in the war and held in temporary camps in Europe. The boy was somewhere in the middle. He was captured late, but he was injured in a way that demanded immediate attention. That combination probably saved his life.
There were also darker aspects of prisoner of war treatment that do not fit the narrative of humane Allied conduct. In some camps, particularly those operated by the French or Soviet forces, conditions were brutal. Prisoners were used for forced labor in dangerous conditions. Food rations were deliberately kept below survival levels.
Medical care was almost non-existent. Thousands of German prisoners of war died in Allied custody after the war officially ended in May 1945. The exact number is disputed, but estimates range from 50,000 to over 100,000 deaths in the year following the German surrender. Most of these deaths occurred in French and Soviet camps, not American or British camps.
But the fact remains that not all prisoners of war were treated according to the Geneva Convention. The boy in this story was fortunate. He was captured by American forces. He received immediate medical treatment. He was transferred to a camp with adequate supplies and professional staff. If he had been captured by Soviet forces on the Eastern Front, his story would likely have ended in the cattle car or in a camp hospital with no morphine, no chest tubes, and no chance of survival.
Context matters, geography matters, timing matters. The boy survived because all three factors aligned in his favor. We are now in May 1945. The war in Europe is over. Germany has surrendered unconditionally. The camps are still full of prisoners of war. But the atmosphere has changed. There is no more combat, no more air raids, no more uncertainty about who is winning.
The allies have won. The prisoners know it. The guards know it. Everyone is waiting for the next phase. Repatriation, release, going home. But for many German prisoners of war, going home is not simple. The boy is still in the camp near a pinnel. He has been there for 6 months. His lung is fully healed. He has no lingering pain or breathing problems.
He has been working in the camp kitchen and occasionally in the supply depot. He has received two letters from his mother in Germany. She is alive. His younger sister is alive. His father is missing. Last seen on the Eastern Front in 1943. The boy does not know if his father is dead or captured or in hiding.
He may never know. That uncertainty is common. Millions of German families are searching for missing sons, fathers, and brothers. The Red Cross is overwhelmed with requests. In late June 1945, the boy and about 500 other prisoners are transferred to a larger camp in Belgium for processing. This is the beginning of the repatriation process.
The allies are releasing prisoners in stages starting with the youngest, the oldest, and those with medical conditions. The boy qualifies on two counts. He is 18 and he has a documented medical injury. He is interviewed by an allied officer who asks him about his military service. When did you join the Vermacht? What unit were you in? Did you participate in any atrocities? The boy answers honestly.
He was conscripted in August 1944. He served in an infantry unit for less than three months. He never fired his weapon in combat. He was captured before he saw any real action. The officer makes notes. No red flags, no war crimes suspected. The boy is cleared for release. In early August 1945, the boy is put on a train heading east toward the French occupation zone of Germany.
The train is crowded but not packed like the cattle car. There are seats. There are windows. There is food and water provided at stops along the way. The journey takes two days. When the train crosses the border into Germany, the boy looks out the window and sees rubble. Entire towns reduced to broken walls and burnt timbers.
Refugees walking along the roads with carts and suitcases. Children sitting in the dirt. The war is over, but the destruction is everywhere. The boy does not know what he is going home to, but he is going home. He is alive. He can breathe. And that after everything is enough. The boy’s survival from a punctured lung in a cattle car during World War II was not a miracle.
It was the result of specific factors that can be understood and analyzed. Let us break them down one more time because they reveal something important about how human beings survive extreme trauma. First, injury severity and location. The shrapnel wound was severe enough to puncture the lung, but not severe enough to sever major blood vessels or cause immediate collapse.
That narrow margin made survival possible. Second, immediate self-care. The boy pressed cloth against the wound and controlled his breathing. Those actions bought him time. Third, young age and physical resilience. An 18-year-old body can compensate for trauma in ways that an older body cannot. Fourth, access to medical care within hours of symptom onset.
The field hospital had the supplies and expertise to perform a chest tube insertion. Fifth, luck. The shrapnel missed his heart. The train was not destroyed in the air raid. The cattle car doors opened before he suffocated. Every one of these factors had to align. Remove any one of them and the boy dies. But there is a broader lesson here. Survival is not random.
It is the product of preparation, decision-making, and context. The boy survived because he made the right choices in the cattle car. He stayed upright. He applied pressure to the wound. He controlled his panic. Those were decisions, not accidents. He also survived because he was captured by Allied forces with functioning medical infrastructure.
That was context, not something he could control. Understanding the difference between what we can control and what we cannot is one of the core lessons of survival in extreme conditions. The boy could control his breathing and his actions. He could not control where the shrapnel hit or who captured him. He maximized the variables he could influence and got lucky on the variables he could not.
That is what survival looks like in war. There is also a psychological dimension. The boy did not give up. He did not scream or thrash or demand help that was not available. He endured. Endurance is not glamorous. It does not make for cinematic moments. It is quiet. It is internal.
It is the decision to keep breathing even when every breath hurts. That decision repeated over and over for three days is what kept him alive long enough to reach the medical tent. Without that psychological resilience, the physical factors would not have mattered. The body follows the mind. When the mind gives up, the body follows. The boy’s mind did not give up.
That is why he is alive to be released in August 1945 instead of buried in an unmarked grave near the French border. There are parts of this story that we do not know and may never know. We do not know the boy’s full name or the exact date he was captured or the specific prisoner of war camp he was held in.
We do not know if he ever reunited with his father or what he did after returning to Germany in 1945. We do not know if he spoke about his experience in later years or if he buried it like so many veterans did. These gaps are frustrating for historians and researchers, but they are also typical. Prisoner of war records from World War II are incomplete.
Many documents were lost, destroyed, or never created in the first place. Personal stories were rarely recorded unless the individual became famous or wrote a memoir. The boy in this story was not famous. He was one of millions. His survival was extraordinary to him and to the doctor who treated him. But in the larger scope of the war, it was just another case file.
We also do not know exactly how many other prisoners of war survived similar injuries under similar conditions. Medical records from Allied prisoner of war camps show that chest wounds were treated regularly, but survival rates were not systematically tracked. We know that pumothorax had a high mortality rate. We know that prisoners of war injured during transport had lower survival rates than those injured in combat and treated immediately.
But we do not have precise numbers for every camp and every injury type. What we do have are individual stories like this one pieced together from medical files, interrogation records, and survivor testimonies. These stories give us a sense of what was possible, even if they do not give us a complete statistical picture. Finally, we do not know how the boy felt about his capttors.
Did he resent the American forces who captured him? Did he feel gratitude toward the doctor who saved his life? Did he blame the Allied pilots who strafeed the train? Or did he understand that they had no way of knowing it was carrying prisoners? These emotional and moral questions are important, but they are rarely documented.
Soldiers and prisoners of war often kept their feelings private. They survived by compartmentalizing. They focused on the immediate task of staying alive and left the larger questions for later. Some of them revisited those questions after the war. Others never did. The boy’s internal world remains unknown. What we do know is that he survived.
And that survival is the thread that ties this entire story together. World War II ended over 80 years ago. The soldiers who fought in it are almost all gone. The prisoners of war who survived the camps are gone. The doctors and nurses who treated them are gone. Within the next few years, there will be no living witnesses left.
That makes stories like this one more important, not less. Because once the witnesses are gone, all we have are the records, the testimonies, and the retelling. If we do not preserve these stories now, they disappear. And when they disappear, we lose something vital. We lose the human detail. We lose the individual choices.
We lose the moments of suffering and resilience that define what the war actually felt like for the people who lived through it. This story matters because it shows us what survival looked like in a specific concrete situation. Not survival as an abstract concept, but survival as a series of small decisions and strokes of luck.
It matters because it reminds us that prisoners of war were not just statistics. They were individuals with names, faces, injuries, and futures. It matters because it documents a level of medical care that was not guaranteed. The boy could have been ignored. He could have been left to die in the cattle car or triaged out of the medical tent as too resource intensive to save.
But he was not. Someone made the decision to treat him. That decision had consequences. It gave him a future. It gave him the chance to go home. It also matters because it complicates the narrative. The allies were not perfect. Prisoner of war treatment was inconsistent. Some camps were well-run. Others were brutal.
Some doctors went above and beyond. Others did the minimum. The boy’s story is an example of the system working. But for every story like his, there are stories of prisoners who were not so fortunate. Recognizing both sides of that reality is important. History is not propaganda. It is not a morality tale with clear heroes and villains. It is messy.
It is contradictory. It is full of people making decisions under pressure with incomplete information. The boy survived because the system worked in his case. That does not mean the system always worked, but it does mean that sometimes it did.